
HKS Basic Level Curriculum
Airway Management
Pre-Hospital Airway Management
Airway management is the most critical intervention in pre-hospital care. Hypoxia kills quickly. As a Basic Level provider, your primary goal is to recognize airway compromise and establish a patent airway using basic maneuvers and adjuncts before progressing to advanced techniques.
Mr. Othman, 52yo
CC: Shortness of breath after eating
Interrogate Patient (AMPLER)
Anatomy of the Airway
The upper airway consists of the mouth, nose, pharynx, and larynx. The most common cause of airway obstruction in an unconscious patient is the tongue falling back against the posterior pharyngeal wall due to loss of muscle tone.
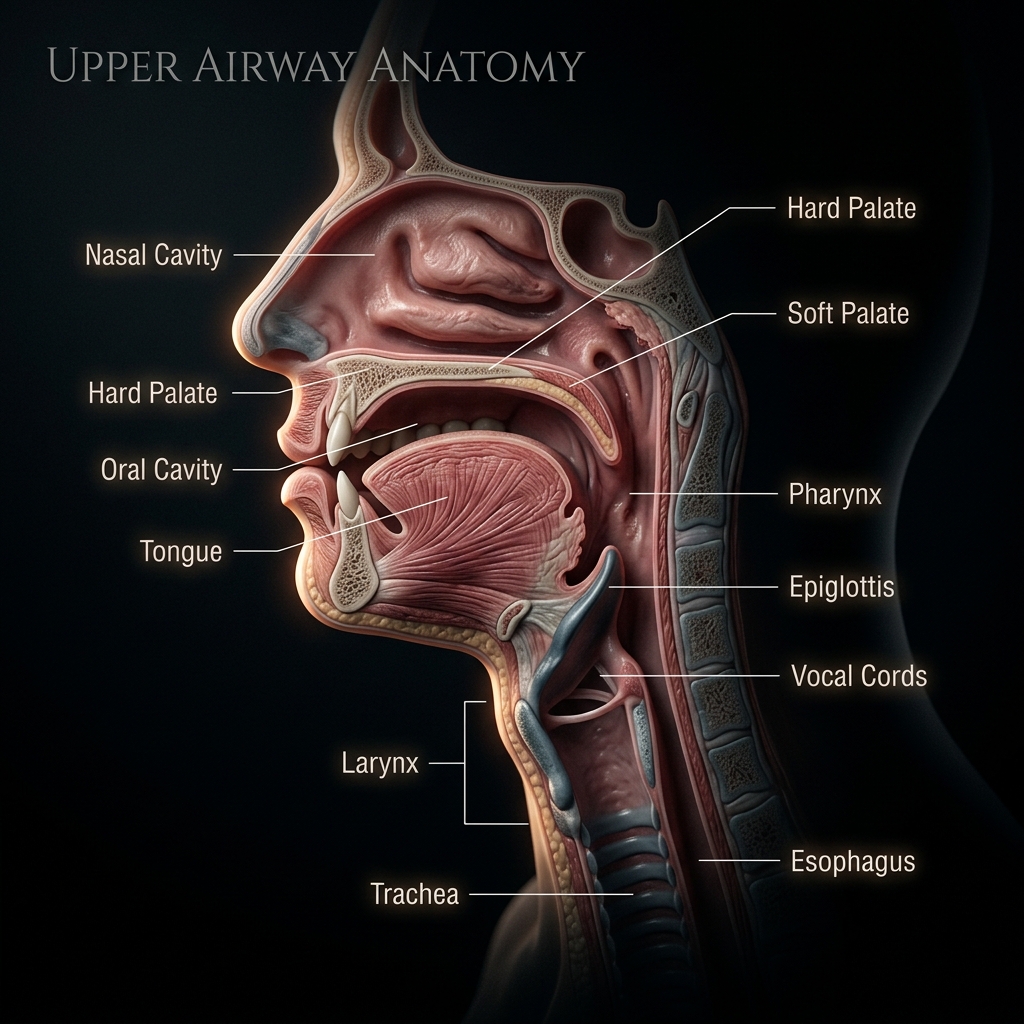
Nasal Cavity
Highly vascularized pathway that warms and filters inspired air.
"NPA insertion route. Must lubricate heavily and insert straight back along the nasal floor with the bevel facing the septum to prevent severe epistaxis."
Avoid NPA in suspected basilar skull fractures to prevent accidental intracranial entry.
FIGURE: Observe the relationship between the tongue, epiglottis, and trachea.
Recognizing Airway Obstruction
Do not rely solely on pulse oximetry (SpO2) to assess the airway. SpO2 is a late indicator of hypoxia. Instead, use the Look, Listen, Feel approach:
- Look: Agitation (early hypoxia), depressed consciousness (late hypoxia), cyanosis, accessory muscle use, seesaw breathing.
- Listen:
- Snoring: Tongue obstruction.
- Gurgling: Fluid (blood, vomit, secretions) in the airway.
- Stridor: High-pitched sound indicating upper airway narrowing (e.g., anaphylaxis, burns).
- Silence: Complete obstruction. This is an immediate life threat.
- Feel: Airflow against your cheek.
A noisy airway is an obstructed airway. A silent airway in an unconscious patient is a dead patient. Act immediately.
Basic Airway Maneuvers
Before using equipment, utilize manual techniques to open the airway.
- Head-Tilt / Chin-Lift: The standard maneuver for medical patients.
- Jaw Thrust: The mandatory maneuver for trauma patients with suspected cervical spine injuries. It lifts the tongue away from the posterior pharynx without extending the neck.
Basic Airway Adjuncts
If manual maneuvers are insufficient or cannot be maintained, use basic adjuncts.
Oropharyngeal Airway (OPA)
- Indication: Unconscious patients with NO gag reflex.
- Sizing: Measure from the center of the mouth (incisors) to the angle of the jaw.
- Insertion: Insert upside down, then rotate 180 degrees once past the soft palate.
Never insert an OPA in a patient with an intact gag reflex. It will induce vomiting, leading to aspiration pneumonitis.
Nasopharyngeal Airway (NPA)
- Indication: Patients with a reduced level of consciousness who still have an intact gag reflex, or patients with trismus (clenched teeth).
- Sizing: Measure from the tip of the nose to the earlobe.
- Insertion: Lubricate heavily. Insert straight back along the floor of the nasal cavity with the bevel facing the septum.
Relative Contraindication: Avoid NPA insertion in suspected basilar skull fractures (e.g., Battle's sign, raccoon eyes, CSF rhinorrhea).
Airway Obstruction
Patent Airway
Upper airway clear. Tidal volume 500ml. PaO₂ 100mmHg. PaCO₂ 40mmHg. Cells receiving adequate oxygen for aerobic metabolism.
Have you mastered this module?