
HKS Basic Level Curriculum
Breathing & Ventilation
Breathing & Ventilation
Once a patent airway is established, you must ensure adequate oxygenation and ventilation. Oxygen is the fuel for cellular metabolism; without it, anaerobic metabolism begins, leading to acidosis and cellular death.
Assessment of Breathing
Assess breathing rate, depth, and effort.
- Normal Rate: 12-20 breaths per minute (adult).
- Bradypnea (< 10 bpm): Often caused by CNS depression (e.g., opioid overdose, head injury). Requires assisted ventilation.
- Tachypnea (> 24 bpm): Often caused by hypoxia, shock, anxiety, or pain.
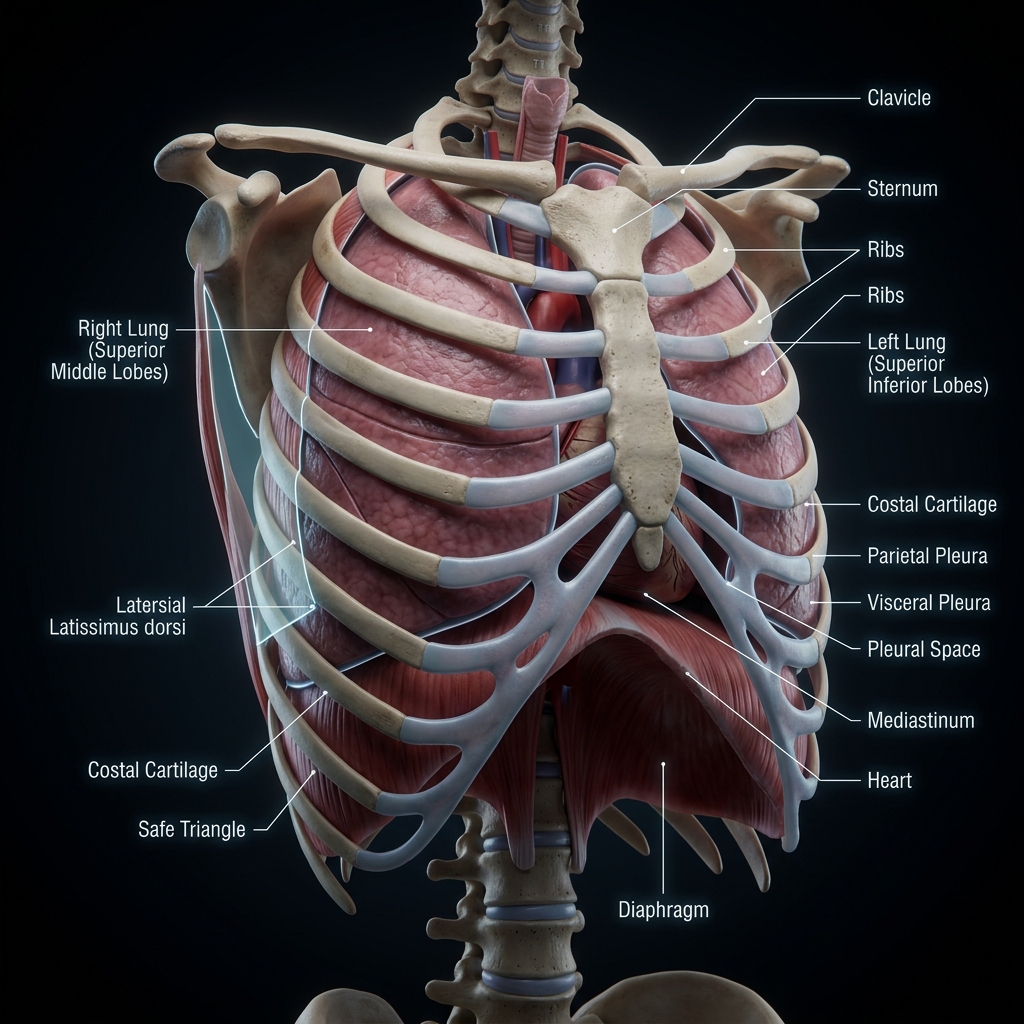
Pleural Space
The potential space between the visceral pleura (lungs) and parietal pleura (chest wall) held together by negative pressure.
"Air accumulation here shifts the lungs and compresses the vena cava, cutting off blood flow back to the heart (Tension Pneumothorax). Must act before cardiac arrest."
Always monitor for signs of tensioning (sudden drop in BP, extreme resistance to BVM ventilations, tracheal shift).
FIGURE: The lungs, pleura, and rib cage mechanics during respiration.
Critical Chest Trauma
In the pre-hospital setting, you must rapidly identify and manage the "Lethal Six" chest injuries, particularly these two that can be managed at the Basic Level:
Tension Pneumothorax
- Pathophysiology: Air enters the pleural space through a one-way valve mechanism (usually a lung laceration) and cannot escape. Pressure builds, collapsing the lung and shifting the mediastinum, which compresses the vena cava and stops venous return to the heart.
- Signs: Severe respiratory distress, hypotension, unilateral absent breath sounds, jugular venous distension (JVD), tracheal deviation (late sign).
- Basic Level Management: High-flow O2, immediate rapid transport. (Decompression is a Master-level skill).
Tension pneumothorax is a clinical diagnosis, NOT a radiological one. Do not wait for an X-ray to suspect it.
Tension Pneumothorax
Simple Pneumothorax
Air enters pleural space through one-way valve defect. Lung begins to collapse on affected side. Mediastinum still midline.
Open Pneumothorax (Sucking Chest Wound)
- Pathophysiology: A defect in the chest wall allows air to enter the pleural space directly from the outside, bypassing the trachea.
- Management: Apply a vented chest seal immediately at the end of exhalation. If a vented seal is unavailable, use a 3-sided occlusive dressing.
If a patient with a chest seal suddenly deteriorates, suspect the seal has caused a tension pneumothorax. Immediately "burp" the seal to release trapped air.
Oxygen Therapy Devices
- Nasal Cannula: 1-4 L/min. Provides 24-36% FiO2. Used for mild hypoxia.
- Non-Rebreather Mask (NRBM): 10-15 L/min. Provides 85-100% FiO2. The standard for trauma, shock, and severe distress. Ensure the reservoir bag is inflated before placing it on the patient.
- Bag-Valve-Mask (BVM): 15 L/min. Used for apneic patients or those breathing < 10 or > 30 bpm with poor tidal volume.
BVM Ventilation Technique
- Use the CE-grip (or two-person VE-grip) to ensure a tight mask seal.
- Ventilate once every 5-6 seconds for adults (10-12 breaths/min).
- Squeeze the bag only until you see visible chest rise. Do not over-ventilate!
Hyperventilation is lethal in trauma and cardiac arrest. It increases intrathoracic pressure, decreases venous return to the heart, and reduces cardiac output. Squeeze the bag gently.
Have you mastered this module?