
HKS Basic Level Curriculum
Common Medical Emergencies
Medical Emergencies & Therapeutics
While trauma is dramatic, medical emergencies make up the majority of pre-hospital calls. Recognition and rapid transport to the correct facility are key.
1. Acute Coronary Syndrome (ACS) / STEMI
ACS involves ischemia (lack of blood flow) to the heart muscle.
- Presentation: Crushing, heavy chest pain, often radiating to the left arm or jaw. Diaphoresis (sweating), nausea, shortness of breath.
- Special Populations: Women, diabetics, and the elderly may have "atypical" presentations (e.g., just sudden weakness, epigastric pain, or isolated shortness of breath).
- Basic Level Management:
- Position of comfort (usually semi-seated).
- O2 ONLY if SpO2 < 94% (Hyperoxia causes coronary vasoconstriction).
- Aspirin 300mg chewed (if not allergic, no active bleeding).
- Rapid transport to a PCI-capable facility.
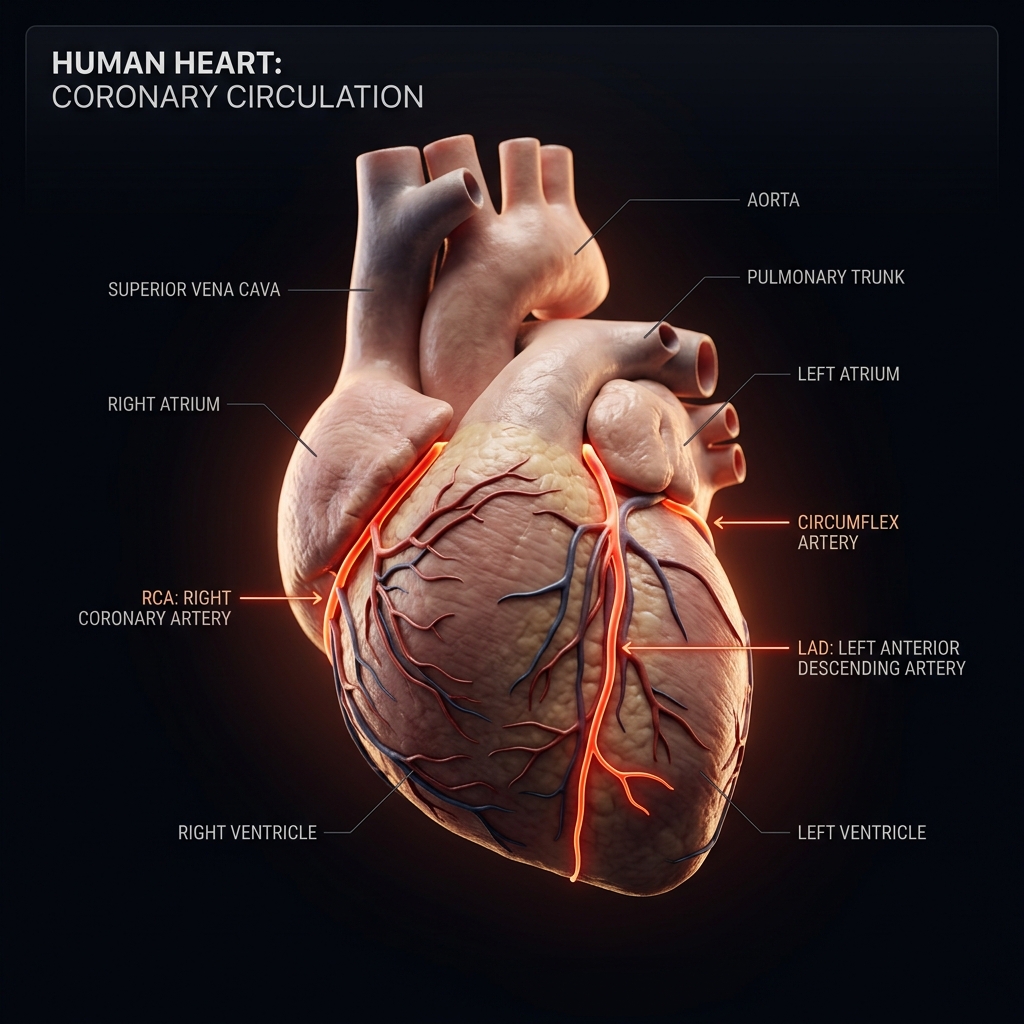
Left Anterior Descending (LAD)
Also known as the 'Widowmaker' artery. Supplies blood to the anterior wall of the left ventricle and septum.
"Occlusion causes massive anterior STEMI (V1-V4). High risk of cardiogenic shock or sudden ventricular fibrillation."
FIGURE: Blockage in the coronary arteries leads to myocardial infarction.
2. Anaphylaxis
A severe, multi-system allergic reaction that is rapidly fatal due to airway swelling and vasodilatory shock.
- Presentation: Sudden onset. Urticaria (hives), swelling of lips/tongue, stridor, wheezing, profound hypotension.
- Basic Level Management:
- Epinephrine (Adrenaline) 1:1000 IM (Intramuscular). This is the ONLY life-saving drug for anaphylaxis. Do not delay.
- Dose: 0.5mg (Adult) via the anterolateral thigh.
- High-flow O2 and fluid resuscitation for shock.
Antihistamines (like chlorpheniramine) do NOT save lives in anaphylaxis. They only treat the rash. Epinephrine is the mandatory first-line treatment to reverse airway swelling and shock.
Anaphylaxis
Antigen Exposure
Allergen enters body. IgE antibodies on mast cells and basophils recognise the antigen. Cross-linking triggers intracellular signalling cascade.
3. Hypoglycemia
Low blood sugar mimicking a stroke, intoxication, or psychiatric episode.
- Presentation: Altered mental status, aggressive behavior, diaphoresis, tachycardia.
- Assessment: Always check a DXT (blood glucose) on ANY patient with altered mental status. Normal is 4.0 - 7.0 mmol/L. < 4.0 is hypoglycemia.
- Basic Level Management:
- If conscious and able to swallow: Oral glucose paste, sweet drinks.
- If unconscious: Do NOT give oral fluids (choking hazard). Requires IV Dextrose or IM Glucagon (Master level). Transport rapidly.
4. Seizures (Status Epilepticus)
- Presentation: Tonic-clonic movements, loss of consciousness, post-ictal confusion.
- Basic Level Management:
- Do NOT restrain the patient.
- Do NOT put anything in their mouth (no bite blocks, no fingers).
- Move dangerous objects away.
- Once the seizure stops, place in the recovery position to protect the airway and administer O2.
- If the seizure lasts > 5 minutes, it is considered Status Epilepticus (a true emergency).
The most critical period of a seizure is the post-ictal phase (after the shaking stops). The brain is exhausted, and the patient may be apneic or have an obstructed airway. Guard the airway closely!
Septic Shock
Infection
Pathogen (bacteria, virus, fungus) invades. Immune recognition via pattern recognition receptors (PRRs). Initial immune response localised.
Have you mastered this module?